
This was a great read. Attia is my kind of doctor, one that challenges the establishment and received wisdom (he was so disillusioned with the medical profession that he left after he graduated, then came back). He explains why & how we must move from treatment-focused care to prevention-focused care.
This was a good complement to the more research-heavy Lifespan, by David Sinclair, which I reviewed here. Santé!
Part I
1: The Long Game
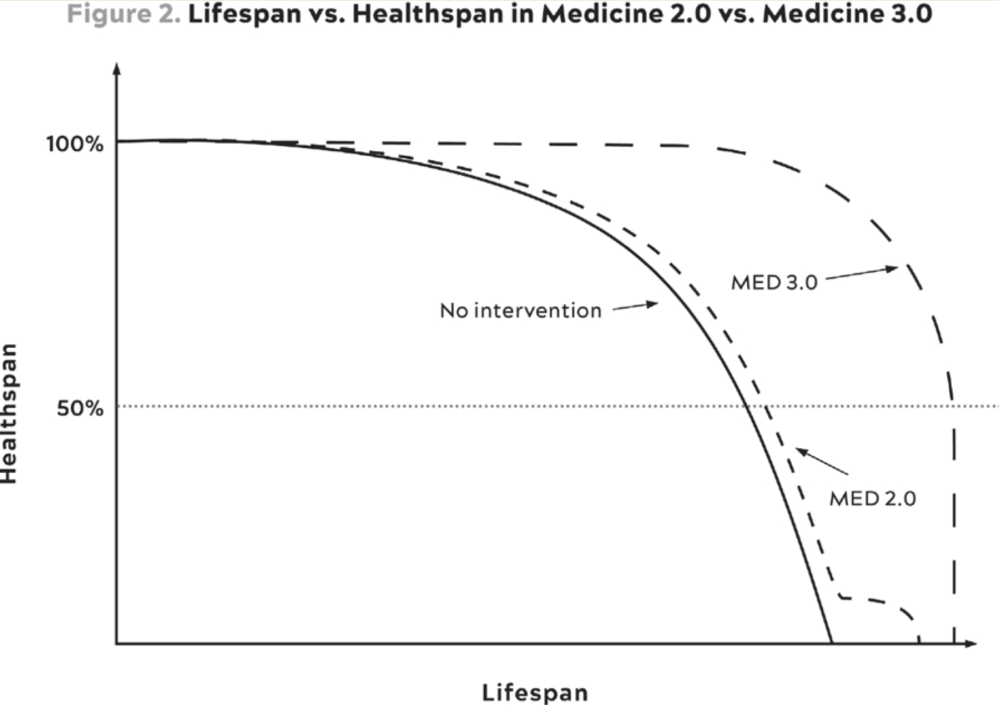
- Lifespan: how long you live. Healthspan: how well you live.
- Four horsemen
- Cardiovascular diseases: mortality cut by 2/3rds in last 60 years
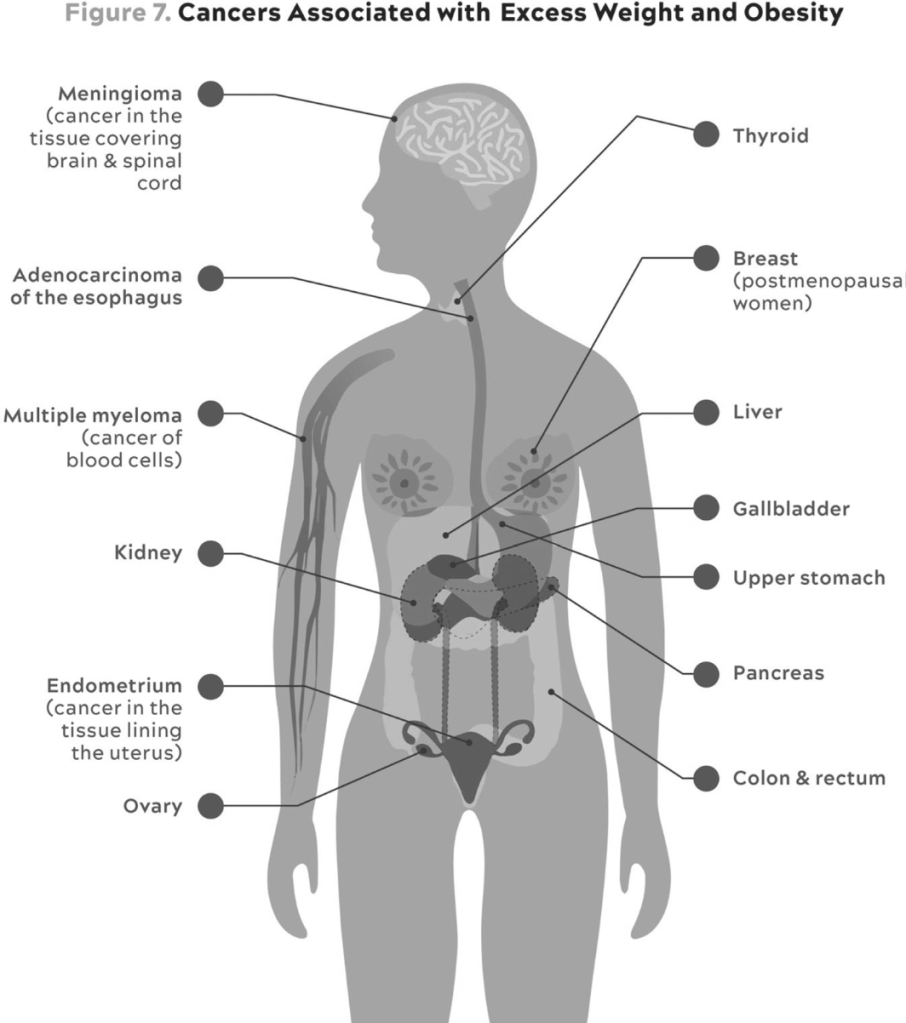
- Cancer: Death rates have hardly changed last 50 years
- Type 2 diabetes: a raging health crisis, very poorly prevented
- Neurodegenerative disease (incl Alzheimer’s): no good treatments
- We need to move to prevention. None of the lung cancer treatments have had as much of an effect as the widespread smoking bans.
- Many medical guidelines are arbitrarily binary: you either are classified to have type 2 diabetes or you don’t, and if you do you get certain treatments. But it’s a spectrum and many treatments should be applied earlier
- “The standard playbook is to wait until someone’s HbA1c rises above the magic threshold of 6.5 percent before diagnosing them with type 2 diabetes.”
2: Medecine 3.0
- “The time to repair the roof is when the sun is shining” – JFK
- “First, do no harm” from Hippocratic oath implies that the best treatment option is the one with the least immediate downside risk / doing nothing, which is not always true
- Medecine 1.0: Hippocrates. Diseases caused by nature and not by Gods.
- Medecine 2.0: 19th century. Germ theory of disease, improved sanitary practices (Pasteur, Lister, Koch). The scientific method (Francis Bacon)
- Containment of HIV and AIDS, recent cure of Hep C
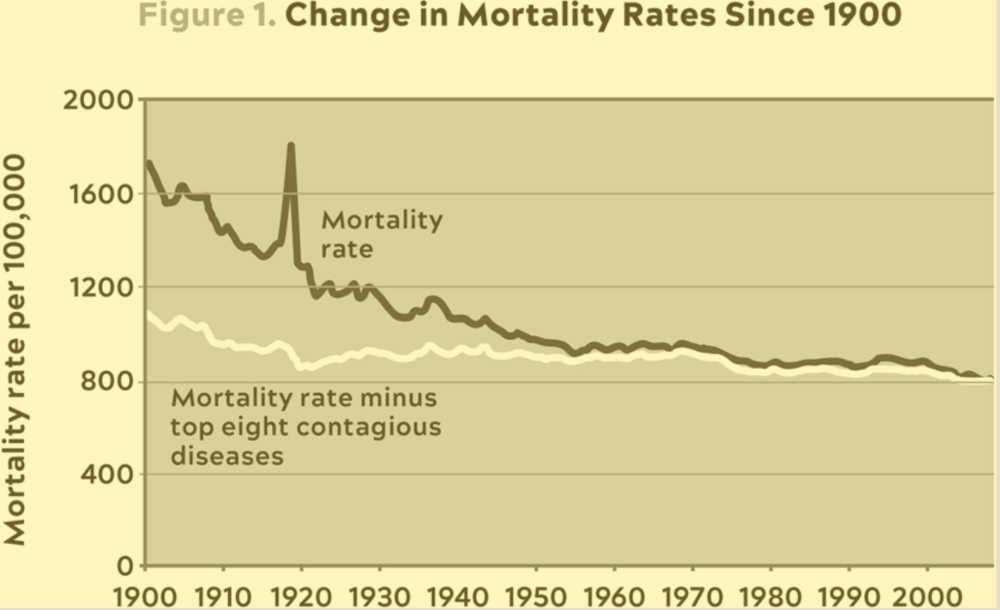
- Most of the progress from Medecine 2.0 against contagious diseases thanks to improved sanitation and antibiotics. Very little progress against the four horsemen.
- Medecine 3.0: greater emphasis on prevention than treatment. Each patient is unique. Acceptance of risk of doing nothing.
- For example, HRT (hormonal replacement therapy) for women became taboo as it caused a slight increase in breast cancer risk, but the absolute risk remained very low. Not considered were the other benefits of HRT (some harder to measure)
- Medecine 2.0 steps in at the end, when your healthspan is already compromised
- Healthspan doesn’t fit into the business model of healthcare in the US. Health insurance company won’t pay a doctor much for them to tell the patient to change what they eat or exercise.
3: Objective, Strategy, Tactics
Medecine 3.0 domains
- Exercise: strength, stability, aerobic efficiency, peak aerobic capacity
- Nutrition: how much you eat (caloric intake) is even more important than what you eat
- Sleep
- Emotional health
- Exogenous molecules: drugs, hormones, supplements.
- Not covered in detail. Attia takes omega-3 fatty acids, vitamin D, magnesium, creatine, electrolytes, and probiotics to support cardiovascular health, bone health, muscle function, hydration, and gut health
- Evidence-based (only do something if passes the gold standard, a randomised controlled trial) -> evidence-informed (accept to take bets, there is no certainty)
Part II
4: Centenarians
- 0.03% of the population live to 100+
- Longevity genes
- APOE gene involved in making a protein that helps carry cholesterol and other types of fat in the bloodstream. Some variants linked to longevity and others with dementia
- FOXO3 gene can be activated/suppressed by our behaviours (eg exercise or slightly deprived of nutrients) and helps keep our cells from becoming cancerous
- Many prevention approaches (exercise, nutrition) overlap for several horsemen
5: Eat Less, Live Longer?
- Rapamycin: compound originally discovered in the soil of Easter Island, used as an immunosuppressant to prevent organ transplant rejection and to treat certain cancers.
- Studies in various organisms, from yeast to mice, have shown that rapamycin can extend lifespan. It does so by inhibiting the mTOR pathway, which is involved in cell growth and aging, potentially mimicking the effects of caloric restriction without the need to reduce food intake.
- The mTOR (mechanistic Target of Rapamycin) pathway is a critical regulator of cell growth and metabolism, influencing aging and longevity through its control over anabolic and catabolic processes.
- Attia takes rapamycin
- Attia is much less excited about Resveratrol and NR than David Sinclair is in Lifespan – my notes here
- Caloric restriction impacts mTOR and AMPK (AMP-activated protein kinase)
- Metformin believed to promote longevity by enhancing insulin sensitivity, reducing inflammation, and activating AMPK
- Protein becomes critically important as we age.
6: The Crisis of Abundance
- Non-alcoholic fatty liver disease (NAFLD), recently renamed metabolic dysfunction-associated steatotic liver disease (MASLD), is a condition marked by excess fat in the liver not caused by alcohol, primarily associated with obesity, diabetes, high cholesterol, or high triglycerides, affecting up to 25% of adults globally
- Metabolic syndrome – a cluster of conditions including high blood pressure, high blood sugar, excess body fat around the waist, and abnormal cholesterol levels, significantly increasing the risk of heart disease, stroke, and diabetes.
- 120M Americans have it! You don’t have to be obese to have metabolic syndrome
- The liver plays a crucial role in managing the body’s metabolic processes, including glucose homeostasis, which is the balance of insulin and glucagon to maintain blood glucose levels

7: The Ticker
- “American women are up to ten times more likely to die from atherosclerotic disease than from breast cancer (not a typo: one in three versus one in thirty). But pink ribbons for breast cancer far outnumber the American Heart Association’s red ribbons for awareness of heart disease among women.”
- LDL (Low-Density Lipoprotein): Often called “bad” cholesterol.
- Function: Transports cholesterol to cells throughout the body.
- Health Risks: High levels can lead to plaque buildup in arteries (atherosclerosis), increasing the risk of heart attack and stroke.
- Foods that Increase LDL:
- Saturated fats: Found in red meat, butter, and full-fat dairy products.
- Trans fats: Found in fried foods, baked goods, and processed snack foods.
- Inflammation is another precursor

What to track
- Apolipoprotein B (ApoB) is vital in lipid transport, forming lipoproteins like LDL that carry cholesterol. Measuring ApoB levels gives a precise count of these particles and helps assess cardiovascular risk.
- Lipoprotein(a), or Lp(a), is a type of lipoprotein similar to LDL cholesterol but includes an additional protein called apolipoprotein(a). Lp(a) can contribute to plaque buildup in arteries, leading to atherosclerosis.
8: The Runaway Cell
“Thanks to better screening and more effective treatments such as immunotherapy, cancer could someday become a manageable disease, perhaps no longer even qualifying as a Horseman.”
9: Chasing Memory
Alzheimer’s risk factors
- APOE-ε4 Allele: Strongest genetic risk factor, with increased risk linked to the number of alleles.
- Familial Alzheimer’s Genes: Early-onset linked to mutations in APP, PSEN1, and PSEN2.
- Non-genetic factors include aging, cardiovascular health, lifestyle choices, head injuries, lower educational attainment, and chronic stress or depression.
- Early signs that hearing loss is a risk factor
Main tools against it
- #1 Exercise
- #2 sleep
Part III
10: Thinking Tactically
First three questions he asks each patient:
- Are they overnourished or undernourished? That is, are they taking in too many or too few calories?
- Are they undermuscled or adequately muscled?
- Are they metabolically healthy or not?
He no longer recommends long fasts due to the impact on undernourishment / muscle loss.
11: Exercise
The most powerful longevity drug.
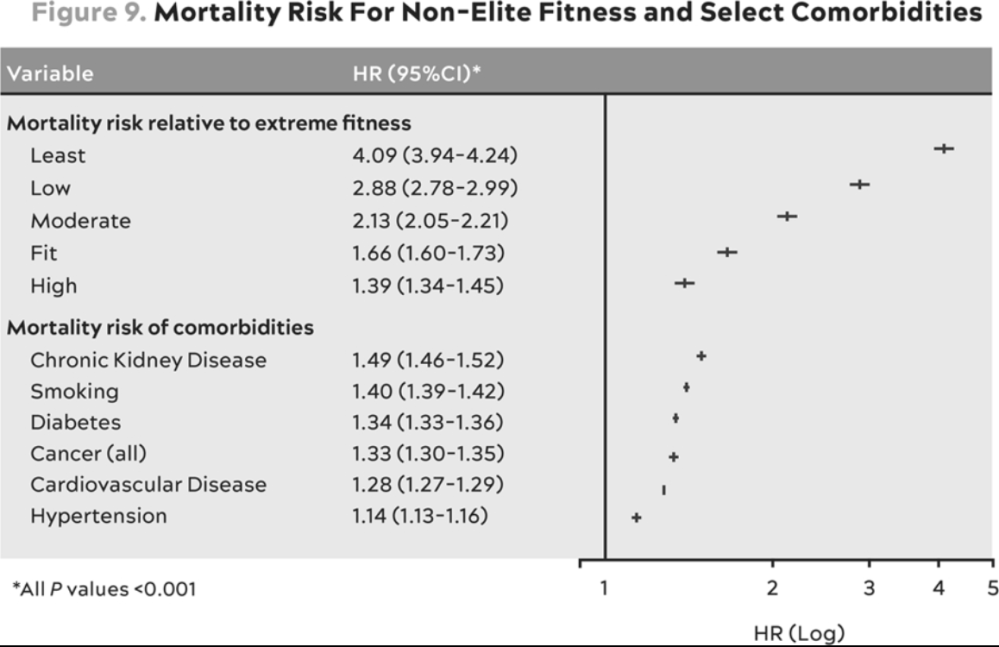
This table expresses all-cause mortality risk (HR = hazard ratio) for different fitness levels compared to individuals in the top 2% of VO2 max for their age and sex (“extreme fitness”) [TOP] and for various comorbidities—that is, people with versus without each illness. [BOTTOM] Kokkinos et al. Link to study
- Undervalued: weight-bearing exercises and strength training increase bone density and muscle mass, reducing the risk of osteoporosis and sarcopenia (age-related muscle loss).
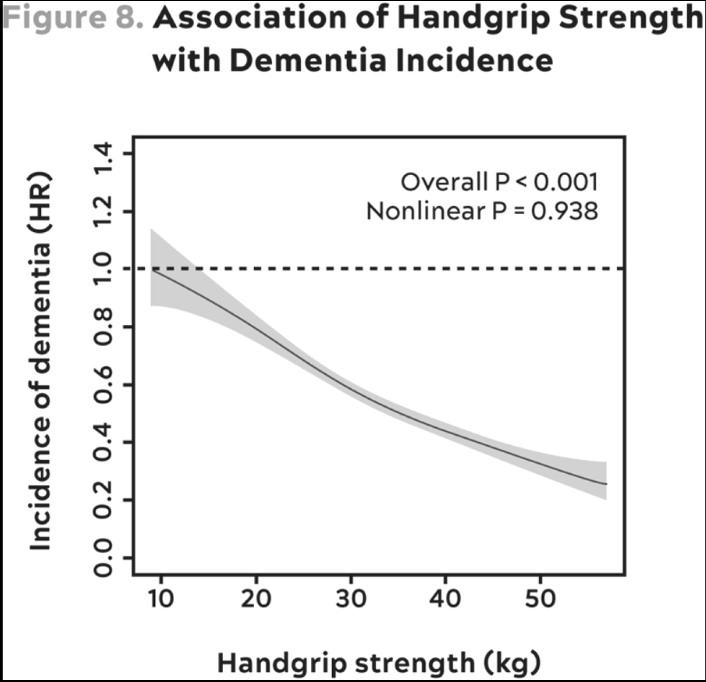
- Regular exercise is associated with better memory, attention, and processing speed, and can help delay the onset of cognitive decline and dementia.
- Regular exercise, particularly endurance training, stimulates the process of mitochondrial biogenesis, leading to an increase in the number of mitochondria in muscle cells. This enhances the cells’ ability to produce energy efficiently.
12: Training 101
Three key things to train on are:
- Endurance & efficiency (cardio)
- Strength
- Stability
- “The healthier and more efficient your mitochondria, the greater your ability to utilize fat, which is by far the body’s most efficient and abundant fuel source. This ability to use both fuels, fat and glucose, is called “metabolic flexibility,” and it is what we want”
VO2 max, or maximal oxygen uptake, is the maximum rate at which an individual can take in and utilize oxygen during intense physical exertion. It is a measure of cardiovascular fitness and aerobic endurance capacity

In addition to muscle mass, bone density declines with age. Important to work on:
- Grip strength. Pull-ups, hanging, deadlifts
- Concentric & excentric loading. eg lifting weight and putting it down. Squats, bench press
- Pulling motions (pulling a weight or resistance towards the body, engaging the back, shoulders, and arms). eg rows, pull-ups
13: The Gospel of Stability
- Injury is a significant reason why many older adults stop exercising.
14, 15: Nutrition
- There is no one-size-fits-all diet; individual responses to diets vary greatly.
- Caloric Balance: Avoid both overeating and under-eating.
- Protein and Essential Fats: Ensure adequate intake of protein and essential fats.
- Saturated Fats (SFA): Found in butter, lard, and coconut oil.
- Monounsaturated Fats (MUFA): Found in olive oil, avocados, and nuts.
- Polyunsaturated Fats (PUFA): Includes omega-3 (EPA, DHA from fish; ALA from flaxseed) and omega-6 fatty acids.
- Micronutrients and Toxins: Obtain necessary vitamins and minerals, and avoid pathogens and toxins.
- Protein is the most crucial macronutrient for achieving health goals, particularly for maintaining muscle mass and metabolic health as we age. Ensure sufficient intake and proper distribution throughout the day.
- In general a lot of BS in nutrutional science
- Inaccuracies in food frequency questionnaires
- Confounding issues
- Not enough randomized trials
16: The Awakening
- Deep NREM sleep is crucial for neurological health, memory consolidation, and clearing out brain waste.
- REM sleep is important for emotional regulation, creativity, and problem-solving.
- As alcohol is metabolized, it disrupts sleep patterns.
- REM Sleep: Reduces the ability to enter REM sleep during the second half of the night.
- Light Sleep: Increases the likelihood of waking up and lingering in light sleep stages.
